Long-read
A traumatic history
Edgar Jones explores the emergence and expansion of the idea of psychological trauma.
Want unlimited, ad-free access? Become a spiked supporter.
Bridging two academic worlds, Edgar Jones is ideally placed to understand the history of psychological trauma. He trained as an economic and social historian at Nuffield College, Oxford, but, as he explains in his office at the Institute of Psychiatry at King’s College London, ‘I always wanted to be a psychotherapist’. This led him to work unpaid as a nursing auxiliary in the department of psychiatry at Guy’s Hospital in London, before using his earnings as a self-employed historian to pay his way through medical school (culminating in a doctorate in clinical psychopathology). And it was at Guy’s that he began to draw upon his undergraduate training to research the history of psychiatry, especially the growing understanding of the psychological effects of conflict. All of which gives Jones a unique insight, as a clinician and a historian, into the development of the idea of trauma.
spiked review: So is it fair to say that up until the mid-19th century, trauma referred almost to a physical wound, rather than a psychic wound?
Edgar Jones: I’d agree with that. It’s towards the end of the 19th century that there’s a shift, with the emergence of the phenomenon of ‘railway spine’. So, due to the increasing number of people involved in railway incidents, doctors noticed that although the physical wound was healing, patients still suffered from other unexplained symptoms, such as poor concentration, headaches, and so on. So they started to wonder if the traumatic effects of a railway accident were not just physical, but psychological, too.
But railway spine remains a fairly marginal condition, because it only affects a small sub-population of railway travellers. Moreover, it is linked to, and understood, in terms of claims for compensation. That’s why as soon as injury compensation for workplace accidents is formalised, so attention focuses on persistent psychological symptoms of traumatic incidents. Indeed, before the First World War, the issue of psychological trauma is almost entirely interpreted in terms of compensation.
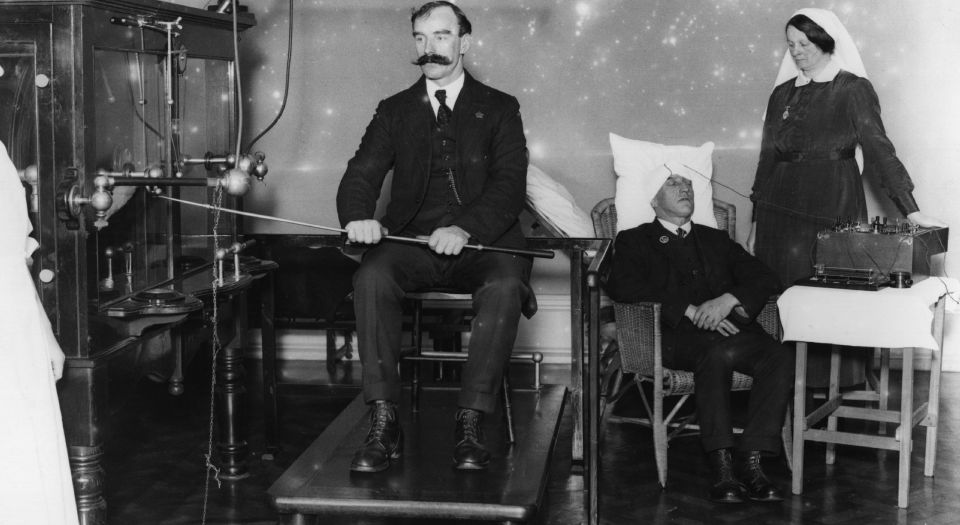
The key turning point is the advent of the First World War, as a result of which you’ve suddenly got large numbers of people suffering from shellshock. Many of them have no individual or family history of mental illness, and a lot of them aren’t physically injured to start with. They’re on the battlefield, but they can’t physically function. So doctors have to think for the first time about what’s really wrong with them, and they conclude that they’re suffering from some sort of psychological trauma.
At the end of 1916, Frederick Mott, a general physician who specialised in psychopathology at the newly established Maudsley Hospital, decided that there were three categories of shellshock victim: those who have had a blow to the head or who have inhaled some toxin, which has had an enduring psychological effect, and they’re a relatively small group; those who are already vulnerable, who have a family or individual history of mental illness that the war has made worse, and this is the largest group; and, this is the interesting part, those, accounting for 20 to 30 per cent of shellshock patients, who have no history of mental illness but go through such an horrific event that it traumatises them. There’s no other explanation for the suffering of this last group, argues Mott, except for their being terrified and exposed to prolonged stress and fear. And Mott reaches that conclusion after the Battle of the Somme, because, by this point, he has seen so many patients – about 5,000 – that he’s able to categorise them, based on detailed records of their family history, medical history and military record.
review: To what extent did the military leadership accept the definition of shellshock?
Jones: At the beginning of the war they were puzzled by it. Still, they took on board the idea of shellshock because they think it’s a physical effect, a form of concussion or some other unknown physiological effect. So the military is willing to tolerate the diagnosis of shellshock. But after the Battle of the Somme, when the casualty numbers are so huge, military leaders become very nervous because they can then see that it’s not a physical effect; it’s either a sign of vulnerability, or something really awful. They’re concerned that it could get out of hand, so they become much less sympathetic.
At this point, there’s a dispute between the psychologically minded doctors who say you have to treat these men, rather than dismiss them as malingerers or cowards, which is what the military tend to say. Military leaders want to say that if you break down with no physical wound, then the problem is one of military discipline. Hence they don’t want to send shellshock sufferers to hospital; they want to send them to a military recuperation camp, where they will rest, do physical exercises, and play games to build up morale.

And so the military set up several convalescent camps along the English coast, to which they send the shellshocked, so as to avoid them being medicalised. But the psychologically minded doctors argued that this isn’t ethical. In their view, these conscripts were suffering just as much as those with bullets in the arm, and you can’t just see them as having weak morale.
review: Beyond the military debates, to what extent does this idea of shellshock enter popular discourse during and after the war? Was it something that civilians talked about?
Jones: Shellshock definitely enters popular culture, because there’s so much of it. I estimate that at least 250,000 soldiers would have been diagnosed with shellshock during the First World War. So it’s common, and it’s a powerful term. People see the effects of it in their relatives when they return home – they’re fatigued and they have these unusual movements. But I don’t think it’s really understood by the general public. There’s a big debate taken up by MPs from about 1916 onwards, because they discover that some of their constituents return to the UK only to be put in lunatic asylums. The MPs counter that these are brave men who shouldn’t be tarred with the stigma of lunacy. So there’s a political campaign to get servicemen out of the asylums and into specialist units, like the Maudsley. This leads to the conversion of hotels and schools into what are designated neurological hospitals.
But once the war is over the public start to switch off from the issue, and the old stigma around mental illness returns, and asylums grow in size throughout the 1920s and 1930s. Shellshock patients begin to get a bit lost in public consciousness up until the the Second World War, when the issue revives.
review: So the idea of trauma at this point still doesn’t have a widespread cultural resonance, and it’s still primarily thought of in terms of a physical injury?
Jones: Yes, in the 1920s and 1930s, trauma is still used to refer to physical trauma. The idea of trauma as a psychic wound develops a little during the Second World War, where there is talk of ‘traumatic neuroses’, but it is quite tightly defined, and is more a psychoanalytic concept than a standard psychiatric one. I have looked through issues of the Lancet and the British Medical Journal published during the Second World War, and the word trauma still has a fundamentally physical meaning. Its emergence as a psychological concept happens during the Vietnam War.

review: So the Vietnam War is the key turning point in the transformation of the idea of trauma?
Jones: Yes, in public consciousness. Because during the Vietnam War, members of the psychiatric community place a huge amount of focus in America on the psychological effects of conflict. Hence post-traumatic stress disorder (PTSD) is first defined in its aftermath in 1980.
The idea of PTSD represents a really significant cultural change. All the way through the Vietnam War, many anti-war campaigners are psychiatrists, psychologists and psychoanalysts, and they contend that despite the US government saying how well troops are being treated, many are coming home and they’re traumatised. PTSD, you see, is presented as something that develops once the prospective sufferer comes home (although it’s now accepted that PTSD exists the moment you are exposed to conflict).
PTSD may not have been recognised by the American Psychiatric Association until 1980, but the campaign was waged during the Vietnam War in the 1970s as a means to show the seemingly real cost of war as being much higher than fatality and casualty figures show. (Just under 60,000 American soldiers were killed in the Vietnam War compared to over 400,000 during the Second World War).
review: It’s noticeable that it’s at this point that the idea of trauma as a psychological wound really starts to gain public traction. For instance, it almost becomes the standard narrative about war – that its effects are deeply psychologically wounding. Think of the movies that emerge at this point, be they Apocalypse Now or The Deer Hunter, which play up the mentally devastating nature of conflict, how it leaves people permanently, psychologically damaged…
Jones: I think it is a progressive development. You do get some of these anti-war movies made in the aftermath of the Second World War, such as The Best Days of Our Lives. It’s an Oscar-winning movie, seen by millions, and it’s about returning servicemen, one of whom has prostheses, another has recurring nightmares and one who has alcohol problems. And it’s made by William Wyler, who himself was a veteran.
It’s a popular movie, which shows that the idea that people are physically damaged and mentally damaged resonates. But the idea of psychological trauma still does not break into the everyday cultural mainstream. What happens with Vietnam – and this is key – is that psychological trauma starts to be applied to civilians in daily life. If I’m in a road traffic accident, or I’m a woman who has been raped, it’s now accepted that I can suffer from PTSD. This wouldn’t have been possible after the First or Second World War. After the Second World War, people accept that soldiers can be psychologically traumatised, but those involved in car accidents are seen as suffering a far less severe form of trauma.
The development and expansion of trauma as a concept that can be applied to daily life proceeds from the Vietnam War onwards, and it’s striking that psychology as an academic and clinical discipline expands at this point, too. During the 1950s and 1960s, psychology is the biggest growing academic discipline, certainly in the UK and the US. Up until then, it was very limited in universities in the 1940s. So there’s a progressive expansion of interest in psychological processes. And popular culture starts to draw on it, too. So, post-Vietnam, there’s an acceptance that we can all suffer from psychological disorders after traumatic events.
review: So you’re saying that the idea of trauma primarily develops in the context of wars, but from the 1970s onwards tends to be applied to everyday life?
Jones: Yes, although there were earlier attempts to apply trauma to everyday life in the 1920s. For instance, in the UK, the Institute of Industrial Psychology was set up in 1921 to look at how the work environment can make you psychologically unwell. But it was a marginal development.
The idea of psychological trauma gets a big boost in the UK in the 1950s with the development of the New Towns, which were planned and built partly as an attempt to improve people’s psychological states, moving people out of urban environments into areas with more space and greenery. But the New Towns’ problem was that they failed to recognise that in the poor housing in East London, from which a sizeable section of the New Towns’ inhabitants came, there were very powerful kinship bonds. Extended families look after each other. So when primarily young people moved to Harlow, for instance, and start having babies they feel lost because their aunts and uncles and grandparents are not there. So they have much nicer houses, but the rates of mental illness go up.
So, the idea of trauma, the idea that events can be psychologically traumatic, always has a context, a frame. To understand a breakdown, for instance, you need to understand the context. What was his or her background, what was their upbringing like, what were the events leading up to it, and what happened afterwards? After the Vietnam War, there’s a recognition that trauma is not something that occurs in isolation. It always has to be framed by context.
review: So there’s nothing automatically traumatising about a given event. What role does the prevailing culture play in creating an expectation that one ought to be traumatised by a given event?
Jones: Yes, there’s nothing automatically traumatising about a given event. If I was on my way home tonight, and someone sprung out in front of me, and threatened me with a knife, I would be frightened. But I wouldn’t necessarily get PTSD. The event in itself is not sufficient to bring on PTSD. A traumatic event is, by its very definition, terrifying, and the worst ones are life-threatening, but it’s what happens next, and the context in which it takes place, which determines whether it triggers an enduring psychological illness. Because it may or may not. For example, some soldiers will break down the very first time they go into battle; some will even break down before they go into battle; and some will go on for weeks before they break down. So there are a lot of complex variables around each individual, which explains the different patterns. They might have been in a similar situation before, and have more coping skills; they might have a very supportive home environment. Trauma is a very nuanced concept. Unlike a physical wound, which is pretty easy to identify and to treat, psychological trauma is not.
review: You mention the role of the frame, of the context. Do you think the narrative of victimhood today does tend to bring with it the expectation that people almost ought to be traumatised by a bad event in their lives?
Jones: I agree. Over the course of the past century, there’s been a cultural switch. During the First and Second World War, you were expected to be resilient, you were expected to be well. And if you were traumatised, you were considered a bit unusual and potentially vulnerable. In wartime, it would be cast as being almost cowardly. Yet, today, we’ve almost gone full circle, and forgotten about the resilient side. Because, in actual fact, most people will not suffer from PTSD if exposed to a terrifying event. If you expose 100 people to the same event, PTSD rates tend to be anything from around three to 15 per cent. So that means 85 per cent of people may be frightened following a terrifying or bad experience, but they won’t get PTSD. They will have natural recovery mechanisms. And that alternative narrative, that awareness of our recovery mechanisms, has tended to be lost.
There is an attempt to recover it with new concepts of post-traumatic growth. Indeed the whole idea of resilience is a relatively new one. The term, resilience, was coined in the 1970s in connection with children who had been fostered or abused in order to describe those who were able to cope and those who weren’t. Resilience was not a term used in the world wars. Everyone was assumed to be tough, so there wasn’t really a word for it. Indeed, at the time, military figures used the term ‘hardening’ – that is to say, military training will ‘harden’ an individual. It will make you a bit tougher.
The word victim would have have had a much narrower meaning in the first half of the 20th century than it does now. Today, anyone who is exposed to a traumatic event is now a victim.
review: Do you think that deeming certain events and experiences as automatically traumatising underpins the automatic labelling of the traumatised as victims?
Jones: Yes, I think that’s right.
Today, the word victim is not a pejorative term – it’s a term of sympathy. Whereas in the 1910s, you could be a victim of a crime, but it would be a neutral term. Likewise, in the war, someone who suffered shellshock was never described as a victim.
We’ve just had the Battle of Passchendaele commemorations, and I was struck by the description of the soldiers who died as victims, and the war as tragic, futile and useless. At the time that was not how people felt at all. The soldiers who survived were very proud of what they’d done. They really did believe that what they were doing was worthwhile, because France had been invaded, Belgium had been invaded, and Germany was not leaving. They saw it as a just war. And, at the time, those who died were described as the glorious dead. Those who died had made a sacrifice that was worthwhile, and were to be commemorated. They were not seen as victims; they were seen as honourable, as courageous. If we’d gone to Tyne Cot Cemetery in the 1920s to commemorate those who lost their lives during the First World War, it would have taken on a very different form than that prevalent today.
As a society, we’ve adopted a blanket view of the First World War, where everyone was traumatised, everyone was a victim. Whereas the real view is a lot more complex. Some people were severely damaged – 250,000 with shellshock were scarred for life. But the vast majority of those who went through it recovered. No doubt they had awful memories, but they continued with their lives. And a lot of them were very proud of their achievements, and felt their military comradeship had been worthwhile. They had beaten this large, professional German army, and they saw this as a considerable, worthwhile achievement.
review: You’ve conducted a lot of research into the explosion of PTSD among soldiers after the Gulf War in 1991, and have noted the role played in this by the fear of chemical and biological weapons, and the lack of conflict experience in a major war since Korea in the 1950s. But what was also interesting was that soldiers were quite willing to talk about being frightened, and to be open to being diagnosed as traumatised – which wouldn’t have been the case in the early 20th century conflicts we’ve mentioned, because of the moral accent on toughness and heroism as opposed to weakness and cowardice…
Jones: Yes, there was an interesting book published recently called Cowardice: A Brief History by Chris Walsh, complete with a suitably yellow cover. Walsh showed that the word cowardice was used a lot in the 19th century, while today its use has narrowed. This is because the space occupied by what is a moral term has been eroded by psychology – that is to say, by a psychological understanding of stressors, vulnerability and all these other variables. You’d be very foolish to accuse a soldier of cowardice on the battlefield now, whereas, during the First World War, generals and officers would quite happily do it, even occasionally shooting people.
review: What do you make of the psychologisation of everyday life, and the use of military metaphors for everyday life, like ‘it’s a warzone’?
Jones: I think we have to be more aware of psychological stress because we all encounter it in our work. And of course the recent developments in terrorism mean that civilians are targets, as we’ve seen recently in London, so some of the pressures that apply to soldiers can apply to anyone close to a terrorist attack.
Indeed, civilians are much more in the firing line today than they were before. In the First World War, civilians were pretty safe. You could be certain that you could survive, although the Second World War is worse.
Civilian life today is far more aware of trauma, because we’re aware we’re under threat from time to time. Travelling on a Tube train, you know there’s a possibility someone might let a bomb off.
review: The role of our contemporary cultural script still seems hugely important here. Far fewer people have died at the hands of terrorists over the past 20 years than in the preceding decades, when in Britain, for instance, the IRA was operative and civilians, as the Guildford and Birmingham pub bombings showed, were as much in the firing line as they are today…
Jones: That’s true. Since 7/7 we’ve had 39 deaths in the UK at the hands of terrorists, which is very small, thank goodness.
review: It shows, I think, that what’s important is not the threat itself, but that people feel far more threatened today. Plus, isn’t it far more acceptable today to be willing to be traumatised, to express one’s vulnerability?
Jones: Stiff-upper-lip culture has definitely been eroded. People are willing to express their feelings. So at an Armistice Day parade, you’ll see grown men crying, and I don’t think you would have seen that in the 1920s and 30s.
The death of Princess Diana was the signal moment in this regard. I can remember watching it on television, and as the car left Kensington Palace, you could hear the sound of people wailing – people who had obviously never met Diana, but who were still in tears. It was acceptable to show your emotions.
review: We’ve talked about the development and expansion of the idea of trauma, from a physical wound to a psychic wound. What do you make of the idea that one can be traumatised by an event that one has not even experienced oneself, for instance, the children and grandchildren of Holocaust survivors?
Jones: There have been quite a lot of conflicting studies of the children of Holocaust survivors. The children appear to be well-adjusted, socially skilled and do as well as children whose parents weren’t in the Holocaust. But I think they’re affected in subtle ways. Anyone who survives the Holocaust must be deeply affected by it. And I think what happens is not that the survivors talk about the trauma, but that their behaviour will somehow be modified. So the children will pick up on this terrible event through their parents’ behaviour. For instance, I heard of a woman in Israel who was with her mother, a survivor, in a supermarket. And the supermarket had sprinklers on because it was so hot. And her mother saw the sprinklers and suddenly thought of gas ovens and had an anxiety attack. And the daughter was there to comfort her. So it is behaviour like that, of people perhaps hoarding food, or insisting on eating everything, that conveys the trauma. Survivors won’t talk about it. Like soldiers, they want to protect their children.
So there is intergenerational transmission of trauma, but it’s done in disguised form. What the veteran and the Holocaust survivor are doing is containing the memory, and if they pass it on, they do so in a modified, mediated way. My father was at Dunkirk, but, when he talked about the war, he never said anything bad about it. He only talked of the positives, the comradeship and so on. It was only when he was in his seventies, and even then I had to press him, that he talked about some of the traumatic things. But by then I was an adult.
review: There is a high moral value attached to suffering today – I just wondered if that plays a role in the willingness to be someone who’s traumatised?
Jones: I’ve done a study of people who fabricate suffering, who claim to be present at a traumatic event. There’s a famous case of a woman who claimed to be in one of the Twin Towers during 9/11 – she even claimed to have a terrible burn on her arm – and her fiance was in the other tower and was killed. And she became a spokesperson for the Twin Towers survivors. This was her undoing, because she was on television, and people recognised her, and revealed that she wasn’t even in America when 9/11 happened. She was a student in Barcelona doing an MBA. She falsified the entire thing.
There’s even cases of people falsifying being involved in atrocities. There was an American soldier who claimed to be involved in an atrocity in the Korean War, went back to a Korean village and apologised to the people. And he’d never been anywhere near the village. There’s something about wanting to be associated with suffering, being part of suffering.
The group which I’ve been researching are much more difficult to detect – people who elaborate their suffering. They’ve been in the war, so they’re genuine veterans, but they haven’t been through the traumatic experience they said they’ve been through. Unlike someone who makes it up, and appears on TV, and is therefore easily exposed, a genuine veteran who claims this or that happened to him is far more difficult to authenticate.
review: Is there now something desirable about being seen as a victim?
Jones: Yes. In the case of this woman who fabricated her experience of 9/11, she had a deep wish to be a prominent victim.
review: Is it because of the greater moral value now attached to suffering that people are willing to fabricate their traumas? Did anything similar happen during the First World War?
Jones: People did fabricate suffering, but mainly for financial gain, because you received a war pension. But what there was far more of was fake heroism. And this, I think, marks a huge cultural shift. The faking in the First and Second World War, centred on being a hero, whereas the focus now is on being a victim, which leads to an increase in cases of fake suffering and psychological injury. There are some cases of veterans today claiming they’ve got PTSD, but, when you investigate, it turns out they haven’t got PTSD, and they weren’t where they said they were, which undermines the importance of the genuine cases.
The idea that you’d fake something like shellshock during the First World War would have been anathema.
Edgar Jones is a professor in the history of medicine and psychiatry at King’s College London.
Picture by: Getty Images.
You’ve hit your monthly free article limit.
Support spiked and get unlimited access.
Support spiked and get unlimited access
spiked is funded by readers like you. Only 0.1% of regular readers currently support us. If just 1% did, we could grow our team and step up the fight for free speech and democracy.
Become a spiked supporter and enjoy unlimited, ad-free access, bonus content and exclusive events – while helping to keep independent journalism alive.
Monthly support makes the biggest difference. Thank you.




Comments
Want to join the conversation?
Only spiked supporters and patrons, who donate regularly to us, can comment on our articles.